How to perform an asymptomatic sexual health screen in primary care: our recommendations
Our most common question received at local and regional testing events is how to perform an effective and appropriate sexual health screen for asymptomatic patients requesting testing. Clearly one option is for those patients to attend our services for review, however we would encourage delivery of asymptomatic screening in other settings – primarily for the convenience of patients.
The information below will help support and inform testing at your service. We are happy to discuss and support any services with testing issues or concerns, as would your local microbiology laboratory.
Please also note that people in England under 25 years old can also get tested as part of the National Chlamydia Screening Programme (NCSP).
Chlamydia
Nucleic acid amplification tests (NAATs) remain the most sensitive and specific test for chlamydia. Testing can be performed on any potential infected anatomical site but routine assessment in primary care requires genital testing only. Depending on the patient’s anatomy the sample to test does vary:
- Vagina – low vaginal swab – a NAAT testing swab applied liberally in and around the vaginal intraiotus for 10 seconds. This sample type will collect cervical discharge and residual urine – the two potential genital sites of infection. This sample can be self-taken.
- Penis– urine sample – a sterile urine pot (without boric acid) should be used to collect a first catch urine sample. The urine should have been held for at least 60, but ideally 90, minutes to maximize NAAT sensitivity. Urethral swabbing for NAATs is not preferred as it confers no improved sensitivity and is more uncomfortable for the patient.
Testing for trans patients
Testing should be adapted according to the anatomy of the patient.
Patients not currently seeking or awaiting reassignment surgery should be tested as above.
Following gender reassignment surgery, and the formation of a neovagina or neopenis, the sample of choice is a first catch urine as the only potential anatomical site for chlamydial infection is the urethra.
Gonorrhoea
Assessment for, and the management of, gonorrhoea is currently recommended to take place in sexual health services in England. This is due to increasing concern over antimicrobial resistance amongst circulating gonorrhoea strains internationally, and also due to the increased chance of false positive results when compared with chlamydia screening.
Currently if you wish to test for gonorrhoea in primary care this can be attempted via direct culture from the affected site[s]: ie. cervix and/or urethra. Specific gonococcal culture should be requested and the sample transported to the lab immediately as Neisseria gonorrhoea is a particularly friable organism.
UPDATE: Following an ongoing and sustained outbreak of gonorrhoea in early 2023 gonorrhoea NAAT testing will now be available for samples sent from primary and secondary care.

Blood testing
NICE guidance recommends that a sexual health screen in England should also include the offer of serological testing for HIV and syphilis.
A common misconception amongst clinicians and patients is that detailed verbal consent is required to perform an HIV test. Whilst this was the case in the 1990s it is no longer the case and is considered a significant barrier to offering testing. Verbal consent is still required but is no more detailed than asking for permission to perform the test, explaining it is a blood test, and how results will be communicated to the patient once they are available.
Further assessment for blood borne virus transmission occurs as part of routine reviews in sexual health services. This can inform a decision in some patients to test for Hepatitis A, B and/or C. If time permits during primary care attendances discussions around common risk factors such as intravenous drug use and endemic sexual contacts.
Window periods
A window period is the time from acquiring infection until a timepoint where its screening test has the highest sensitivity.
- For chlamydia infection this time is 2 weeks.
- For HIV and syphilis serology this window is currently 4-6 weeks.
Serological testing currently has a 99% sensitivity at 6 weeks, and close to 100% sensitivity at 3 months.
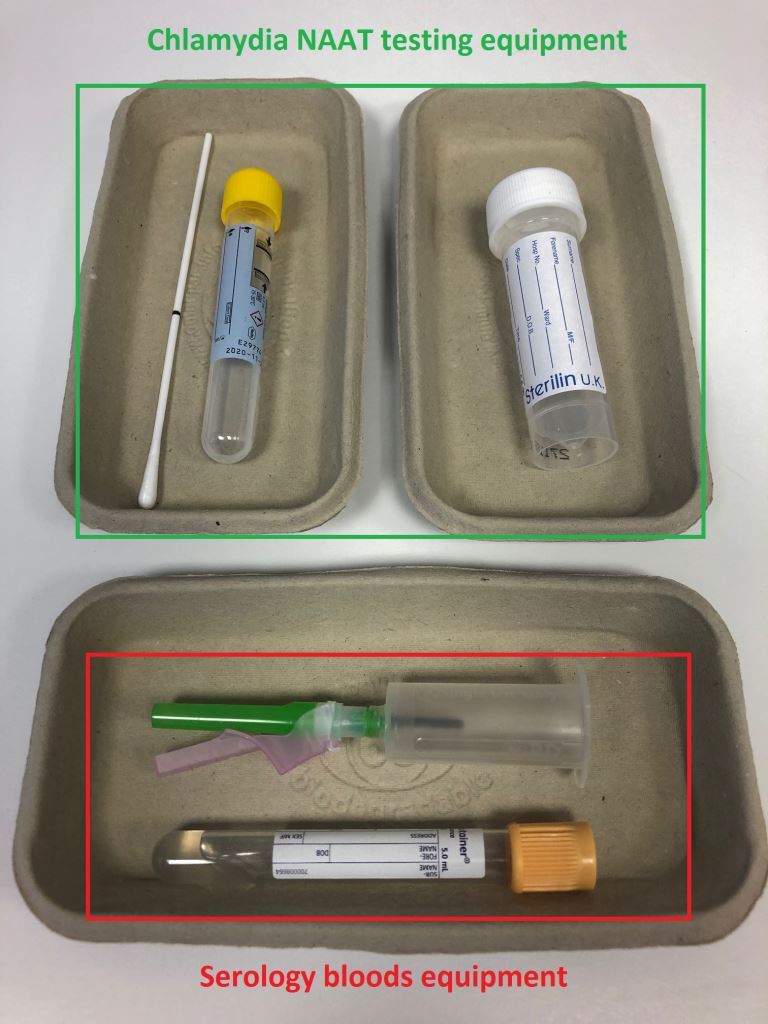
Testing equipment
Frequently asked questions about
STI screening in primary care
-
You mention “potential anatomical sites” for chlamydia NAAT testing…. what does this refer to?
Although not marketed for use outside of the genitalia chlamydia NAAT tests have an increasingly robust evidence base for their use at extragenital sites. This is of particular importance for screening men-who-have-sex-with-men (MSM) where >50% of diagnosed STIs occur outside of the genitals. NAAT testing can also be utilised in potential cases of chlamydial conjunctivitis after semen splashes to the eye.
-
Can we access gonorrhoea NAAT testing in primary care?
At present this is not available but early work is being carried out with local labs to see if gonorrhoea testing can be introduced into primary care sourced NAAT samples in the future. We will keep you updated on these discussions.
-
Is there benefit in testing patients within the window period?
Testing is almost always helpful if a patient is within the window period. A test does not always miss an active infection during the window, but will have increasing sensitivity as each day passes until the completion of the window period. Testing can be offered for patients in this time, but they should be recommended to repeat testing once the window period has fully elapsed.
-
What should I do if I get a positive HIV or syphilis result back?
Our first suggestion would be to review the lab report which often contains detailed information from local microbiology, and often a helpful recommendation of the action to take. A further phone call to the lab can also be helpful. The next stage is then usually a call through to ourselves to discuss the case, including how to manage disclosure to the patient. We are always happy to provide support.
-
Where would you class as endemic contacts?
This definition changes frequently based on international epidemiology data, primarily via WHO recommendations. As a broad rule sexual contacts born in and/or living for a prolonged period in Eastern Europe, Russia, Asia, the Middle East, Africa, the Caribbean, Central and South America can be considered as higher risk for the acquisition of blood borne viruses – primarily Hepatitis B and HIV, with some countries also high risk for Hepatitis C.
Reliable data on HIV prevalence rates per country is available here.
-
Any other top tips for testing?
Be aware that NAAT collection tubes have an expiry date. They will not be accepted and processed by the lab if tubes have expired. Ensure regular review and stock rotation of your testing equipment.